Robotics Series · Healthcare
Intuitive da Vinci 5 Deep Dive: Surgical Robotics, Hospital ROI, Pricing, Adoption, and Deployment Strategy
A business-focused deep dive on Intuitive da Vinci 5, covering surgical robotics, hospital adoption, pricing context, operating-room workflow, training, service economics, data, force feedback, and what leaders should verify before investing in robotic surgery.
Intuitive da Vinci 5 belongs in this robotics series because it represents one of the most mature commercial robotics categories in the world: robot-assisted surgery. It is not a warehouse robot, not a humanoid, and not an autonomous machine replacing a professional. It is a precision platform that helps highly trained surgeons perform complex minimally invasive procedures through robotic instruments, 3D visualization, software, workflow design, and hospital support infrastructure.
This is the final deep dive in Black Scarab's robotics series. Spot and ANYmal showed inspection. Digit, Figure, Atlas, Optimus, and G1 showed different humanoid paths. Universal Robots showed collaborative arms. Amazon Proteus showed autonomous movement inside logistics. da Vinci 5 shows a different lesson: some of the most valuable robots do not remove the expert from the loop. They amplify the expert.
This article belongs to the Top 10 Robots Transforming the World in 2026 series. Read it beside NVIDIA's physical AI stack, Roboflow's computer vision platform, Prophesee's event-based vision layer, and Hailo's edge AI acceleration layer to connect surgical robotics with compute, vision, low-latency sensing, and efficient edge inference.
For business leaders, da Vinci 5 is useful because the buyer is not a hobbyist or a factory manager. The buyer is a hospital, health system, surgical department, or ambulatory surgery strategy team. The evaluation is not only technical. It involves capital planning, surgeon adoption, operating-room throughput, patient volume, clinical governance, service contracts, instrument utilization, training, credentialing, and long-term program economics.
Executive Summary
da Vinci 5 is Intuitive's fifth-generation multiport surgical robotics platform. Intuitive positions it as the successor to its established da Vinci ecosystem, with more than 150 design innovations, 10,000x the computing power compared with da Vinci Xi, and improvements across surgeon control, visualization, ergonomics, data, software, and workflow. Its most notable new capability is force feedback, which Intuitive describes as measuring force at the instrument tip and feeding that information back to the surgeon.
The system matters commercially because Intuitive is not selling a one-off machine into an experimental market. da Vinci is a mature surgical robotics ecosystem with a large installed base, recurring instruments and accessories, service revenue, surgeon training, hospital programs, procedure growth, and a long history of minimally invasive surgery adoption.
For non-technical executives, the simplest framing is this: da Vinci 5 is not a robot surgeon. It is an operating-room platform. The business case depends on whether a hospital can build enough qualified procedure volume, surgeon adoption, OR workflow discipline, service support, and patient demand around the system to justify the capital and recurring cost.
da Vinci 5 at a Glance
What is it?
Practical Answer
A robot-assisted surgical platform for minimally invasive procedures performed by trained surgeons.
Who is it for?
Practical Answer
Hospitals, health systems, surgical centers, and surgical teams building or expanding robotic surgery programs.
What makes da Vinci 5 different?
Practical Answer
Force feedback, upgraded computing and imaging, improved ergonomics, broader data capabilities, and workflow improvements compared with prior da Vinci generations.
What does it not do?
Practical Answer
It does not make surgical decisions independently, remove the need for trained surgeons, or automatically guarantee better outcomes.
How should leaders evaluate it?
Practical Answer
By procedure volume, surgeon adoption, specialty fit, OR utilization, total cost, service support, training, patient demand, and measurable program outcomes.
| Question | Practical Answer |
|---|---|
| What is it? | A robot-assisted surgical platform for minimally invasive procedures performed by trained surgeons. |
| Who is it for? | Hospitals, health systems, surgical centers, and surgical teams building or expanding robotic surgery programs. |
| What makes da Vinci 5 different? | Force feedback, upgraded computing and imaging, improved ergonomics, broader data capabilities, and workflow improvements compared with prior da Vinci generations. |
| What does it not do? | It does not make surgical decisions independently, remove the need for trained surgeons, or automatically guarantee better outcomes. |
| How should leaders evaluate it? | By procedure volume, surgeon adoption, specialty fit, OR utilization, total cost, service support, training, patient demand, and measurable program outcomes. |
What da Vinci 5 Actually Does
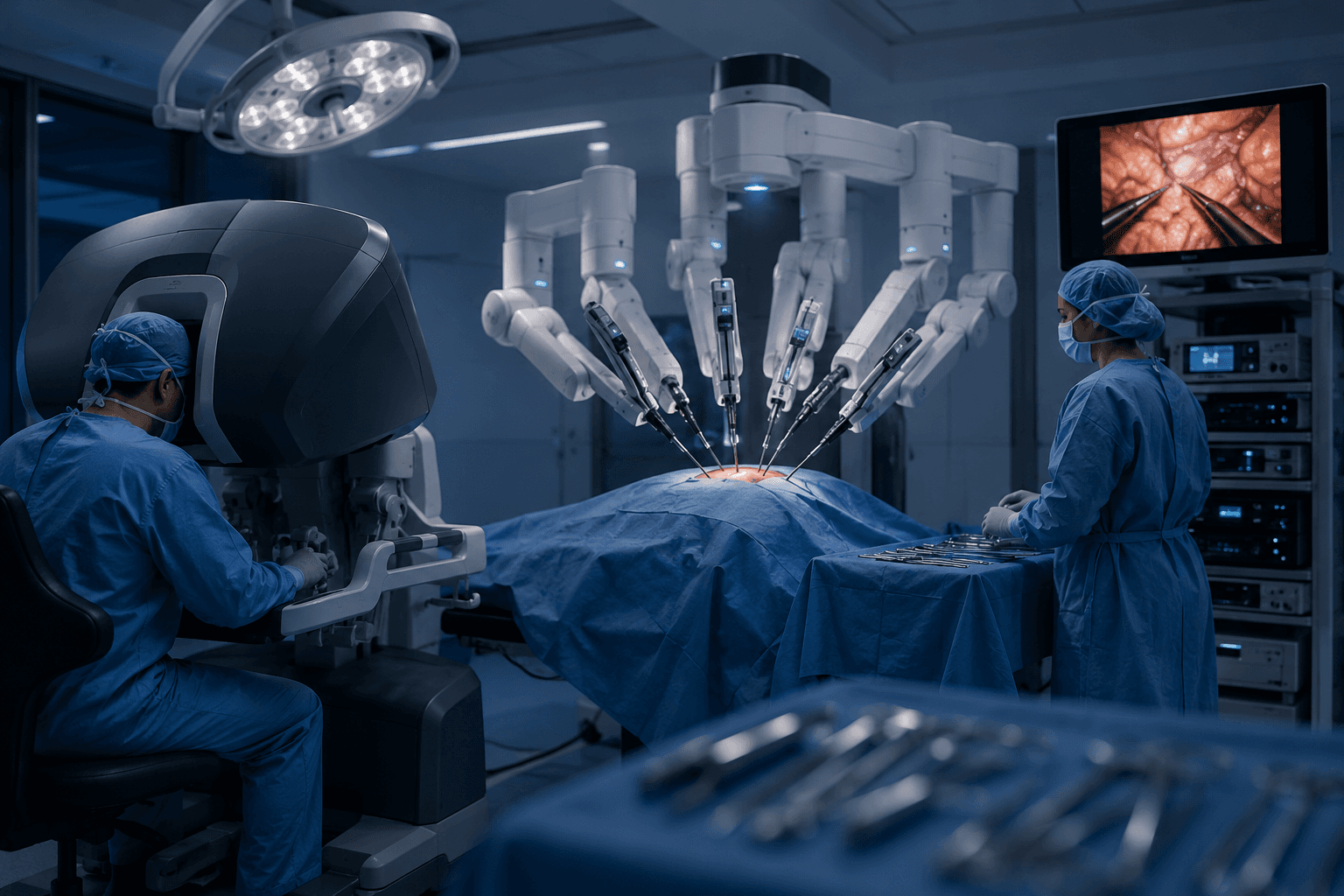
A da Vinci procedure is still surgeon-controlled. The surgeon sits at a console and controls instruments inside the patient through small incisions. The system translates hand movements into precise instrument motion, provides magnified 3D visualization, filters tremor, and gives the surgeon a more controlled interface for complex minimally invasive work.
da Vinci 5 adds an important sensory layer: force feedback. In traditional minimally invasive surgery, surgeons often have reduced tactile feel compared with open surgery. Intuitive says da Vinci 5 measures force at the instrument tip and feeds that information back to the surgeon. The business significance is not a flashy robot trick. It is about giving a skilled professional another stream of useful information during delicate work.
The platform also matters as a system of systems. A da Vinci 5 deployment includes the patient-side robotic system, surgeon console, vision system, instruments, accessories, software, training, service support, OR workflow, sterile processing, scheduling, and data. The visible robot arms are only the most obvious part of a much larger surgical program.
Why Surgical Robotics Is Different
Most robots in this series are judged by how much work they can perform on their own. Surgical robotics is different. The highest-value part of the workflow is still human expertise: anatomy knowledge, judgment, planning, risk management, decision-making, and accountability. da Vinci's role is to make that expertise easier to apply through a precise robotic interface.
That distinction matters for executives. A hospital should not evaluate da Vinci 5 like a labor-replacement robot. It should evaluate it like a clinical platform, a service line investment, and an operating-room capability. The question is not 'How many surgeons can this replace?' The question is 'Can this help our surgical teams deliver more minimally invasive procedures, attract and retain surgeons, support patient demand, and build a stronger robotic surgery program?'
This is also why surgical robotics has been commercially durable. Hospitals do not buy only the robot. They buy into a procedural ecosystem: surgeon training, instruments, imaging, service, data, workflow, and brand recognition around robotic-assisted surgery.
Adoption and Market Maturity
da Vinci is one of the clearest examples of robotics moving from early adoption into a mature commercial category. Intuitive's 2025 annual report cites more than 20.4 million cumulative procedures performed using Intuitive systems through 2025, more than 12,100 total systems installed globally, and more than 11,100 da Vinci systems at customer sites. It also reports that by the end of 2025, customers had installed more than 1,200 da Vinci 5 systems and used them in more than 270,000 procedures.
The adoption pattern matters. A new humanoid robot might still be trying to prove one repeatable use case. da Vinci is operating in a market where hospitals already understand robotic surgery as a competitive and clinical program area. In 2025, da Vinci procedures increased to more than 3.1 million. The challenge is no longer simply explaining what surgical robotics is. The challenge is proving the next system can improve workflow, surgeon experience, program economics, and procedural capability enough to justify an upgrade or expansion.
da Vinci 5 also launched through a staged rollout. That is normal in high-stakes medical technology. Hospitals need training, support, procedure coverage, regulatory clarity, inventory planning, and workflow readiness before a new platform scales broadly. For buyers, staged adoption is a reminder that availability and clinical clearance are not the same thing as instant operational readiness.
Why da Vinci 5 Is Commercially Mature
Large installed base
What It Means for Business Leaders
Hospitals are not evaluating surgical robotics as a brand-new category; many are expanding or upgrading established programs.
Recurring revenue model
What It Means for Business Leaders
Instruments, accessories, service, and utilization matter as much as the initial hardware purchase.
Procedure ecosystem
What It Means for Business Leaders
Value depends on surgeon adoption, specialty mix, patient volume, training, and OR workflow.
Regulated product category
What It Means for Business Leaders
Deployment depends on clearances, indications, clinical governance, and institutional protocols.
Platform competition
What It Means for Business Leaders
Hospitals can use robotic surgery capability as part of recruitment, service-line strategy, and patient-facing positioning.
| Signal | What It Means for Business Leaders |
|---|---|
| Large installed base | Hospitals are not evaluating surgical robotics as a brand-new category; many are expanding or upgrading established programs. |
| Recurring revenue model | Instruments, accessories, service, and utilization matter as much as the initial hardware purchase. |
| Procedure ecosystem | Value depends on surgeon adoption, specialty mix, patient volume, training, and OR workflow. |
| Regulated product category | Deployment depends on clearances, indications, clinical governance, and institutional protocols. |
| Platform competition | Hospitals can use robotic surgery capability as part of recruitment, service-line strategy, and patient-facing positioning. |
Where da Vinci 5 Fits in Healthcare
da Vinci systems are used across multiple surgical specialties, including urology, gynecology, general surgery, thoracic surgery, colorectal surgery, and other procedure areas depending on local regulatory clearance, hospital capability, and surgeon training. da Vinci 5 has also received additional clearance for certain cardiac procedures, expanding the strategic conversation beyond the original launch scope.
The best way to think about da Vinci 5 is as a platform for high-value professional work. Surgical procedures are complex, expensive, capacity-constrained, and reputation-sensitive. A hospital does not need a robot because robots are fashionable. It needs a robotic surgery platform when the procedure mix, surgeon base, patient demand, and financial model support it.
The strongest fit is usually a hospital or health system with enough surgical volume to keep the system utilized, enough trained surgeons to avoid single-operator dependency, and enough operational discipline to prevent the robot from becoming an underused prestige purchase.
Healthcare Use Cases to Evaluate
Urology
Business Question
Is robotic surgery already central to the service line or patient demand?
Why It Matters
Urology has been one of the most visible robotic surgery categories and can anchor volume.
Gynecology
Business Question
Can the hospital support minimally invasive procedures with trained teams and efficient scheduling?
Why It Matters
Program value depends on clinical fit, case mix, and operating-room execution.
General and colorectal surgery
Business Question
Are there enough complex minimally invasive cases to justify dedicated robotic capacity?
Why It Matters
Procedure mix and surgeon adoption determine utilization.
Thoracic and cardiac
Business Question
Does the hospital have the specialist expertise and governance needed for advanced use cases?
Why It Matters
High-complexity specialties require careful training, credentialing, and support.
Ambulatory strategy
Business Question
Can robotic procedures move into lower-acuity settings without compromising safety or economics?
Why It Matters
Site-of-care strategy can reshape utilization, but only when clinical and operational requirements are met.
| Area | Business Question | Why It Matters |
|---|---|---|
| Urology | Is robotic surgery already central to the service line or patient demand? | Urology has been one of the most visible robotic surgery categories and can anchor volume. |
| Gynecology | Can the hospital support minimally invasive procedures with trained teams and efficient scheduling? | Program value depends on clinical fit, case mix, and operating-room execution. |
| General and colorectal surgery | Are there enough complex minimally invasive cases to justify dedicated robotic capacity? | Procedure mix and surgeon adoption determine utilization. |
| Thoracic and cardiac | Does the hospital have the specialist expertise and governance needed for advanced use cases? | High-complexity specialties require careful training, credentialing, and support. |
| Ambulatory strategy | Can robotic procedures move into lower-acuity settings without compromising safety or economics? | Site-of-care strategy can reshape utilization, but only when clinical and operational requirements are met. |
Pricing and Total Cost
Intuitive does not publish a simple online checkout price for da Vinci 5. That is expected for a regulated surgical robotics platform. Hospitals usually evaluate these systems through direct commercial engagement, institutional procurement, financing, trade-in or upgrade paths, service terms, instruments, accessories, training, and procedure-volume planning.
Public financial filings are still helpful because they show the economic structure. da Vinci systems are capital equipment, but the long-term economics include recurring instruments and accessories used in procedures, annual service contracts, software and workflow support, and hospital operating costs. In other words, the purchase price is only the front door.
A hospital should model da Vinci 5 as a program, not a device. The real total cost includes the system, instruments, sterile processing, OR time, training, case scheduling, service, downtime risk, staff coverage, surgeon onboarding, marketing, and governance. The system only makes sense when procedure volume and program design can carry those costs.
da Vinci 5 Cost Areas to Budget For
Capital system cost
What It Covers
Robot platform, console, vision stack, installation, accessories, and configuration.
Buyer Note
Final pricing should be verified directly with Intuitive and compared against upgrade, lease, or financing options.
Instruments and accessories
What It Covers
Procedure-specific tools, sterile accessories, replacement cycles, and case-level consumables.
Buyer Note
Per-procedure economics matter because high utilization also drives recurring cost.
Service and uptime
What It Covers
Maintenance, support, repairs, updates, and service coverage.
Buyer Note
Downtime can disrupt surgical schedules, so service terms are part of the ROI.
Training and credentialing
What It Covers
Surgeon onboarding, OR team training, proctoring, simulation, and internal governance.
Buyer Note
A robot without trained teams is expensive idle capacity.
Program operations
What It Covers
Scheduling, room turnover, sterile processing, staff allocation, reporting, and patient flow.
Buyer Note
Operational discipline determines whether robotic surgery scales or bottlenecks the OR.
| Cost Area | What It Covers | Buyer Note |
|---|---|---|
| Capital system cost | Robot platform, console, vision stack, installation, accessories, and configuration. | Final pricing should be verified directly with Intuitive and compared against upgrade, lease, or financing options. |
| Instruments and accessories | Procedure-specific tools, sterile accessories, replacement cycles, and case-level consumables. | Per-procedure economics matter because high utilization also drives recurring cost. |
| Service and uptime | Maintenance, support, repairs, updates, and service coverage. | Downtime can disrupt surgical schedules, so service terms are part of the ROI. |
| Training and credentialing | Surgeon onboarding, OR team training, proctoring, simulation, and internal governance. | A robot without trained teams is expensive idle capacity. |
| Program operations | Scheduling, room turnover, sterile processing, staff allocation, reporting, and patient flow. | Operational discipline determines whether robotic surgery scales or bottlenecks the OR. |
Treat public pricing references as directional only. da Vinci 5 procurement should be quoted directly with Intuitive and evaluated through a hospital-specific total cost model.
The ROI Logic
The da Vinci 5 ROI question is not simple because hospitals are not measuring one factory task. They are balancing clinical capability, procedure volume, surgeon preference, patient demand, OR throughput, service-line growth, recruitment, reimbursement, capital budgets, and competitive positioning.
A strong business case starts with utilization. How many cases can realistically move to the platform? Which specialties will use it? How many surgeons are trained or willing to train? How much OR time will robotic cases require? Can the hospital run enough cases per week to avoid underutilization?
The strongest ROI cases are usually programmatic. A hospital develops a robotic surgery service line, trains multiple surgeons, standardizes workflows, measures outcomes and costs, improves scheduling, manages instrument use, and expands volume over time. The weakest case is buying the system because competitors have one, without a real plan to fill it.
da Vinci 5 ROI Checklist
What procedure volume will move to the platform?
Why It Matters
Robotic surgery economics depend heavily on utilization and case mix.
How many surgeons will actively use it?
Why It Matters
A single champion surgeon is not the same as a resilient hospital program.
Can OR workflows support the system?
Why It Matters
Room setup, turnover, instruments, staffing, and scheduling affect throughput.
What are the measurable clinical and operational goals?
Why It Matters
Hospitals should track outcomes, complications, conversion rates, length of stay, case time, and cost per case where appropriate.
How will recurring costs be controlled?
Why It Matters
Instruments, accessories, service, and utilization discipline shape long-term economics.
| Question | Why It Matters |
|---|---|
| What procedure volume will move to the platform? | Robotic surgery economics depend heavily on utilization and case mix. |
| How many surgeons will actively use it? | A single champion surgeon is not the same as a resilient hospital program. |
| Can OR workflows support the system? | Room setup, turnover, instruments, staffing, and scheduling affect throughput. |
| What are the measurable clinical and operational goals? | Hospitals should track outcomes, complications, conversion rates, length of stay, case time, and cost per case where appropriate. |
| How will recurring costs be controlled? | Instruments, accessories, service, and utilization discipline shape long-term economics. |
The Technology Stack Behind da Vinci 5
da Vinci 5 is useful for Black Scarab because it shows how robotics becomes valuable when hardware, software, data, workflow, and human expertise are designed together. The robot arms are only one layer.
At the hardware layer, the system includes robotic arms, surgical instruments, endoscopic imaging, the surgeon console, controllers, cameras, displays, and operating-room equipment. At the software layer, it includes motion control, visualization, instrument management, data capture, training support, and workflow features. At the business layer, it includes service contracts, clinical programs, regulatory compliance, and institutional governance.
The most interesting strategic direction is data. Surgical robotics platforms can become structured data platforms for procedure analysis, training, workflow improvement, and future AI-assisted features. That does not mean autonomous surgery is around the corner. It means the operating room is becoming more instrumented, measurable, and software-defined.
What a da Vinci 5 Deployment Really Includes
Robotic platform
Examples
Patient-side system, robotic arms, console, vision cart, surgical instruments.
Business Question
Does the platform fit the hospital's procedure mix and OR footprint?
Clinical workflow
Examples
Room setup, docking, instrument flow, anesthesia coordination, turnover, scheduling.
Business Question
Can the OR team run robotic cases efficiently and safely?
Training and governance
Examples
Surgeon training, credentialing, simulation, proctoring, case review, quality metrics.
Business Question
Does the institution have a durable robotic surgery program, not just equipment?
Data and software
Examples
Procedure data, system logs, imaging, workflow metrics, analytics, updates.
Business Question
Can data improve training, utilization, and program management?
Support ecosystem
Examples
Service, instruments, accessories, sterile processing, spare planning, vendor support.
Business Question
Can the hospital maintain uptime and predictable case economics?
| Layer | Examples | Business Question |
|---|---|---|
| Robotic platform | Patient-side system, robotic arms, console, vision cart, surgical instruments. | Does the platform fit the hospital's procedure mix and OR footprint? |
| Clinical workflow | Room setup, docking, instrument flow, anesthesia coordination, turnover, scheduling. | Can the OR team run robotic cases efficiently and safely? |
| Training and governance | Surgeon training, credentialing, simulation, proctoring, case review, quality metrics. | Does the institution have a durable robotic surgery program, not just equipment? |
| Data and software | Procedure data, system logs, imaging, workflow metrics, analytics, updates. | Can data improve training, utilization, and program management? |
| Support ecosystem | Service, instruments, accessories, sterile processing, spare planning, vendor support. | Can the hospital maintain uptime and predictable case economics? |
How to Pilot or Upgrade Into da Vinci 5
A hospital evaluating da Vinci 5 should begin with a service-line plan, not a technology demo. The right first question is which procedures, surgeons, and patient populations justify the investment. The second question is whether the institution can operate the program consistently.
For hospitals already using da Vinci systems, da Vinci 5 is an upgrade and expansion question. Leaders should compare the existing installed base, surgeon demand, case backlog, room utilization, training needs, and trade-in or financing options. The decision may be less about whether robotic surgery matters and more about which generation and capacity level best supports the program.
For hospitals building a first robotic surgery program, the bar is higher. They need physician champions, executive sponsorship, operating-room readiness, credentialing standards, case-volume assumptions, patient-safety governance, and a financial model that includes recurring costs.
da Vinci 5 Deployment Roadmap
1
Action
Define the service-line strategy.
Success Signal
Target specialties, procedure volume, surgeon demand, and patient demand are clear.
2
Action
Model total cost by procedure.
Success Signal
Capital, instruments, accessories, service, staffing, and OR time are included.
3
Action
Build surgeon and OR team readiness.
Success Signal
Training, credentialing, scheduling, and clinical governance are planned before go-live.
4
Action
Start with defined procedures.
Success Signal
Initial cases are selected for clinical fit, team readiness, and measurable program value.
5
Action
Track utilization and outcomes.
Success Signal
Leaders monitor case volume, OR time, complications, conversions, length of stay, cost per case, and surgeon adoption where appropriate.
6
Action
Expand only with evidence.
Success Signal
Additional rooms, surgeons, or specialties are added after utilization and workflow justify scaling.
| Step | Action | Success Signal |
|---|---|---|
| 1 | Define the service-line strategy. | Target specialties, procedure volume, surgeon demand, and patient demand are clear. |
| 2 | Model total cost by procedure. | Capital, instruments, accessories, service, staffing, and OR time are included. |
| 3 | Build surgeon and OR team readiness. | Training, credentialing, scheduling, and clinical governance are planned before go-live. |
| 4 | Start with defined procedures. | Initial cases are selected for clinical fit, team readiness, and measurable program value. |
| 5 | Track utilization and outcomes. | Leaders monitor case volume, OR time, complications, conversions, length of stay, cost per case, and surgeon adoption where appropriate. |
| 6 | Expand only with evidence. | Additional rooms, surgeons, or specialties are added after utilization and workflow justify scaling. |
When da Vinci 5 Is a Bad Fit
da Vinci 5 is a bad fit when a hospital lacks procedure volume. A surgical robot with low utilization becomes a capital-heavy symbol rather than a productive platform. If there are not enough surgeons, cases, or service-line demand, the economics become difficult.
It is also a bad fit when leadership expects the robot to solve process problems by itself. Poor scheduling, weak sterile processing, inconsistent OR staffing, slow room turnover, limited training, and unclear governance can make robotic surgery more expensive and less efficient.
Finally, da Vinci 5 is a bad fit when the hospital treats technology adoption as a marketing exercise. Robotic surgery should be evaluated through patient safety, clinical appropriateness, surgeon capability, operational readiness, and transparent economics. The robot is powerful, but the institution still has to run the program.
Black Scarab Takeaway
Intuitive da Vinci 5 is one of the most important robots in this series because it shows what robotics can become when a company builds not only hardware, but an entire commercial and clinical ecosystem around a high-value professional workflow.
For industry leaders outside healthcare, the lesson is broader than surgery. The future of robotics will not only be autonomous machines replacing people. Some of the biggest categories will be expert-assist platforms that give professionals better control, better data, better visualization, and better workflow.
For Black Scarab's catalog vision, da Vinci 5 is a reminder that the real basket is always bigger than the robot. A surgical robotics deployment includes cameras, instruments, compute, displays, software, data systems, service, sterilization, training, safety governance, and workflow integration. The robot is the visible product. The operating model is the business.
Sourcing & Verification
This guide was compiled using Intuitive's official da Vinci and da Vinci 5 product materials, Intuitive investor and annual reporting, FDA clearance announcements, and public company materials around patient reach, system placements, procedures, and robotic surgery program economics. This article is a business strategy overview, not medical advice. Hospitals should verify indications, regulatory status, pricing, clinical claims, service terms, training requirements, and patient-safety protocols directly with Intuitive, clinical leadership, legal counsel, and qualified medical professionals before procurement or deployment.
Email Updates
Stay current on edge AI and physical AI
Get thoughtful Black Scarab updates on edge AI platforms, real-world deployments, and the systems moving AI into the physical world.
No hype. Just useful updates on real-world AI systems.
Related Insights
Healthcare
Case Study #9: Medtronic GI Genius and Edge AI for Real-Time Colonoscopy Detection
A real-world look at how Medtronic's GI Genius intelligent endoscopy module uses edge AI to support real-time polyp detection, improve adenoma detection rates, and reduce missed lesions during colonoscopy.
Read related insight
Healthcare
Case Study #6: Mount Sinai & Butterfly Network – Edge AI for Point-of-Care Diagnostics
A real-world look at how Mount Sinai and Butterfly Network used handheld, edge-enabled imaging to extend diagnostic capability into rural, low-resource, and emergency care environments.
Read related insight
Construction
OpenSpace Deep Dive: Construction Reality Capture, Visual Intelligence, and the Built-World Data Layer
A business and investor deep dive on OpenSpace, the construction visual intelligence platform turning jobsites into searchable, measurable, AI-ready records for owners, general contractors, trades, insurers, and infrastructure operators.
Read related insight
Next Step
Design a healthcare system around your own care environment
If you are evaluating edge AI for diagnostics, monitoring, or care delivery, we can help scope the right combination of devices, compute, and deployment strategy.